
Authored by Nicholas Oliver Corey Kuzik
Reviewed by Stephen Carrell, PGY-4 at University of Alberta
Edited and posted by Yosra Er-reguyeg
April 12, 2026 | 5 min

Before diving into the essentials of a physical exam, a quick review from last month. A thorough history taking from your patient may sound something like:
Example of a systematic history:
Hello, my name is Corey one of the med students working with the ophthalmology team. Which eye is bugging you? What are you noticing in that eye specifically - entire field loss/blurriness or part of the vision missing and where? Has the other eye had any problems? When did this all start? Has this happened before? What were you doing when it started? Has it been getting worse or has it been stable? Any other symptoms (pain, photophobia, headache, dizziness, peripheral neurological changes)? Medications changes? PMHx FHx and on and on.
If that makes sense, then read on to learn about the physical exam. If it doesn’t make sense, then maybe read last month's post on taking a systematic history. If it still doesn’t make sense after reading last month’s post, maybe take a nap. Don’t sleep on…well… sleep in this case I suppose.
Physical Exam
Three things are essential to measure: vision, pupils, and pressure (THE EYE VITALS). Even outside of your ophthalmology elective, if you are working with a team that wants to consult ophthalmology, these are three things you MUST measure to help the consult: vision, pupils, and pressure.
Pro Tip: Some also consider extraocular movements and confrontational visual fields as the remaining eye vitals. Be prepared to tell the consultant your findings with these too.
These are also the three things you must measure before dilating the eyes. Dilation can skew near vision, pupil assessment, and pressure measurements, and can even be dangerous if you haven’t checked the pressure first.
Vision conventionally means visual acuity, but to help me remember I stack some extra things into vision: acuity (central vision), confrontational field (peripheral vision), ocular motility & alignment (resting and moving vision), and color vision (neurological vision).
Visual Acuity (distance central vision): Recorded as 20/XX for each eye. If they can't see the big "E" (20/200), you can still quantify their visual acuity, and move down the chain:
Confrontational Visual Fields: Test the four quadrants. This relies on intense eye contact, bonus points if you have dreamy eyes. Sit 1 metre away from the patient, who is occluding one eye, close your opposite eye (patient closes right eye, you close left eye). Get them to look deeply into your open eye, asking them to not break eye contact or cheat. Ideally, you and the patient should be able to count fingers in each of the 4 quadrants of both eyes (See below). Ensure you hold your hand about midway as they count your fingers.

Extraocular Alignment and Movements
Starting with alignment, determine if there is asymmetry in alignment between the two eyes. Then have the patient follow your finger in the 6 cardinal positions of gaze (see below). Also, note any diplopia and pain due to looking in any of the cardinal positions.
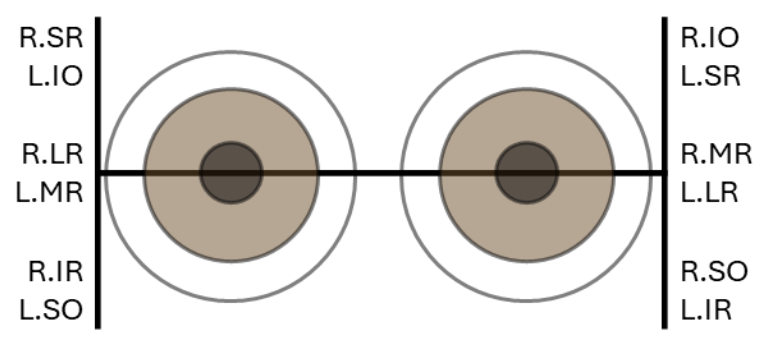
Don’t worry about the acronyms for now, but know that the 6 cardinal positions of gaze can help pinpoint specific muscles and nerves on both eyes.
Colour Vision
Using pseudoisochromatic plates, such as the Ishihara plates, record the fraction of plates the patient correctly identifies (e.g., 10/17). Plate instructions may also indicate the potential colour defect.
2. Pupils: PERRLA-DC
Checking to ensure the Pupils are Equal and Round in a lit and dim room, as well as Reactive to Light and Accommodation-Direct and Consensual in a dim room.
The RAPD (Relative Afferent Pupillary Defect): Light should make pupils constrict, and if shining light in an eye causes it dilate…well thats abnormal. Use the swinging flashlight test to shine light in one eye, and bounce to the other eye. Do this again and again. If the affected pupil paradoxically dilates when light shines on it, (and other eye has no consensual constriction), this suggests a RAPD (See below). (more on this in a future blog post!)

The Dilation Decision: The "Point of No Return"
You have now performed all the physical exams that must be conducted before administering dilating drops. Stop and think. Before dilating, run this safety checklist:
The Drops: Typically, you’ll administer a combination of Tropicamide (parasympatholytic) and Phenylephrine (sympathomimetic). Patients with darker irises have more pigment to "soak up" the medication and may require an extra round of drops compared to those with lighter eyes.
Slit Lamp
Even if you aren't dilating, you can do most of this. If you are dilating, wait about 15–20 minutes for the drops to "cook" before trying to see the back. Move systematically from the front of the eye to the back:
Simple Tips for Med Students to Get a Fist Bump: Comment on whether the chamber looks “shallow” or “deep”. If you see high pressures (IOP) and a shallow chamber, you’re looking at a major risk factor for Acute Angle Closure Glaucoma. Mentioning this will likely get you a fist bump.
When examining the retina, comment on:
There are two main ways to conduct a fundus exams:
Putting It Together
A strong presentation shows you’ve synthesized the data from the history and the physical:
“This is a 28-year-old with a history of recurrent cold sores, presenting with 2 days of a painful, red right eye and significant photophobia. Vision is 20/40 in the right eye and 20/20 in the left. Pupils are equal, round, and reactive to light and accommodation both direct and consensual. Pressure is 15. On slit lamp, with fluorescein staining I appreciated a branching dendritic ulcer with terminal bulbs. I’m concerned about HSV and recommend starting acyclovir. I would not recommend topical steroids as this could worsen the infection”.
That’s a strong presentation. Even if the diagnosis ends up being ophthalmia nodosa from a seemingly friendly fuzzy caterpillar.
Common Pitfalls
Final Thought: A good exam isn't about seeing everything perfectly the first time. It’s about being reliable, systematic, and safe. Speed and efficiency comes later.
Next month:
Vision Loss on Your Ophthalmology Elective


