
Authored by Nicholas Oliver Corey Kuzik
Reviewed by Stephen Carrell, PGY-4 at University of Alberta
Edited and posted by Yosra Er-reguyeg
June 27, 2026 | 5 min
Red eye feels like it should be simple. When my eyes get red, it’s a good indicator to stop studying and go to sleep. But the red eyes you see will not be this simple…well, hopefully. Otherwise, who referred this person?!
Red eye is more complicated because many different structures on or around the eye can make it look red when they are irritated, inflamed, infected, injured, or under pressure. That’s a lot of real estate, including the eyelids, conjunctiva, sclera, cornea, anterior chamber, iris, and orbit.
Conjunctivitis can cause a red eye. So can dry eye, subconjunctival hemorrhage, episcleritis, scleritis, keratitis, uveitis, acute angle-closure glaucoma, trauma, chemical injury, endophthalmitis, and more!! Some of those are common and self-limiting. Some are sight-threatening. Some are common enough and dangerous enough that you need to pause before saying “probably pink eye” and moving on with your day.
As a medical student, your job is not to perfectly diagnose every red eye from across the room. Your job is to collect the right information, recognize danger, and present the case in a way that helps the resident or staff make decisions quickly.
For red eye, the main question is:
Is there something here that could threaten vision, or is this a lower-risk red eye?
That means while examining the eye in a structured way, you should be mindful of some key history cues, signs, and symptoms that act as red flags.
History:
Signs:
Symptoms:
A painless red eye with normal vision is usually less scary.
A painful red eye with decreased vision is not something to casually call conjunctivitis. That eye demands attention.
The History That Matters
Vision
If they report visual disturbances, ask how long they have had vision that is blurry, dim, distorted, or missing. Does anything make it better or worse (e.g., posture, time of day, exercise)?
Pain
Ask what kind of pain it is. Mild irritation or gritty discomfort fits with conjunctivitis, dry eye, or blepharitis. Severe pain, deep/piercing pain, pain with headache or nausea, or pain with reduced vision should make you slow down.
Photophobia
Photophobia is high yield, but not specific. In a red eye, it should raise concern for corneal involvement or intraocular inflammation, especially keratitis or anterior uveitis. It can also occur with ocular surface disease, including dry eye, so the symptom alone does not make the diagnosis.
The key is that photophobia should make you slow down. If light hurts, especially in a unilateral red eye, do not be too reassured by a relatively quiet-looking conjunctiva. Check the cornea with fluorescein, look for ciliary flush, and assess the anterior chamber for inflammatory cells if you can.
Contact Lenses
Ask every patient with red eye if they wear contacts. If yes, ask:
A painful red eye in a contact lens wearer is keratitis or corneal ulcer until proven otherwise. Especially if they sleep, swim, or shower in their lenses. Getting a contact lens history can quickly move a case from confusing to a slam dunk.
Trauma and Chemical Exposure
Ask directly. Patients may not mention the “small” thing that hit their eye, the piece of metal they were cutting, the tree branch that snapped back, or the cleaning product that splashed.
If there is chemical exposure, irrigation comes first. Try to find out if it was an acid (e.g., battery acid) or base (e.g., ammonia).
If an open globe is possible, as a medical student you should not check pressure.
Recent Surgery or Injection
Recent eye surgery or intravitreal injection should sound alarms. Pain, redness, and decreased vision after an intraocular procedure is endophthalmitis until proven otherwise.
Discharge and Itching
This helps once the dangerous stuff is less likely.
Discharge does not save you from doing the rest of the exam. A red eye with discharge can still have corneal involvement.
The Red Eye Exam: As Always, Start With Vision, Pupils, and Pressure
For red eye, it is tempting to jump straight to the slit lamp. I get it. You finally feel like you locked in on appreciating cell and flare, and you want to flex. But every good eye exam should start with:
1. Vision
Always check visual acuity first. A red eye with normal vision is usually less concerning. A red eye with reduced vision moves higher on the danger list. Check each eye, with correction if available, and use pinhole if they didn't get down to 20/20.
2. Pupils
Check whether the pupils are equal, round, reactive, and whether there is an RAPD. Then look at the shape. A small or irregular pupil can fit with uveitis. A mid-dilated, poorly reactive pupil with pain, cloudy cornea, and elevated IOP should make you think about acute angle closure. An abnormal pupil is not just a random exam finding. It changes the differential.
3. Pressure, If Safe
Measure IOP if there is no concern for open globe. This caveat matters. If the story suggests penetrating trauma or ruptured globe, do not check pressure and do not press on the eye. If it is safe, pressure can be extremely helpful. High IOP in a painful red eye pushes acute angle closure much higher on the list.
What if you suspect an open globe injury?
Look for obvious clues like a peaked pupil, irregular globe contour, hyphema, uveal prolapse, or severe vision loss after trauma. Shield the eye and escalate immediately. If there is concern for a subtle wound leak but no obvious globe rupture, a Seidel test can help find a leak.
Red Eye: Location, Location, Location
Once you have vision, pupils, and pressure, move from outside to inside.
External Exam
Check for:
This is where you catch the red eye that is not just a red eye. Orbital cellulitis, thyroid eye disease, carotid-cavernous fistula, exposure keratopathy, herpes zoster ophthalmicus, cranial nerve problems, and eyelid malposition can all start making noise here.
Lids, Lashes, and Lacrimal System
Look for crusting, blepharitis, hordeolum, trichiasis, entropion, discharge, or a foreign body hiding under the lid. If the patient has foreign body sensation, evert the lid. Eyelids are sneaky. They can hide the thing that keeps scratching the cornea.
Conjunctiva and Sclera
Now ask: what kind of red is it? Is this a sharply demarcated subconjunctival hemorrhage? Diffuse conjunctival injection? Ciliary flush? Sectoral redness? A deeper, more violaceous redness? A painless, bright red patch with normal vision suggests subconjunctival hemorrhage. Diffuse injection with watery discharge may fit viral conjunctivitis. Ciliary flush should make you think about deeper inflammation, such as keratitis, uveitis, or acute angle closure. Deep, piercing pain with tenderness should make you think about scleritis.
Cornea
Look for:
If the cornea is not clear, or you see an irregular corneal light reflection, slow down. A painful red eye with corneal opacity or infiltrate is not routine conjunctivitis.
Fluorescein
Use fluorescein to look for epithelial disruption. Specifically looking for:
A corneal infiltrate plus epithelial defect should make you think about infectious keratitis or corneal ulcer. A branching dendrite should make you think about herpetic keratitis.
Anterior Chamber
Is it deep or shallow? Is there cell or flare? Is there blood? Is there pus? A shallow chamber with high pressure supports acute angle closure. Cell and flare suggest intraocular inflammation. Hypopyon after cataract surgery should sound the alarms for endophthalmitis.
High-Yield Differential by Pattern
Now that you have a structured history and exam, the differential becomes easier.
1. Painless, Bright Red Patch, Normal Vision, +/- spontaneous
Think: subconjunctival hemorrhage.
This looks dramatic but is often benign. Ask about trauma, eye rubbing, coughing, vomiting, heavy lifting, anticoagulants, hypertension, and recurrence. If there is pain, reduced vision, or trauma, stop treating it as simple.

Subconjunctival hemorrhage, the patient is on anticoagulant medication. Photo by Stephan Moll, MD, StatPearls Publishing LLC, CC BY-NC-ND 4.0.
2. Itchy, Bilateral, Watery Eyes
Think: allergic conjunctivitis.
Itching is the key feature. Not “a bit itchy.” More like, “I want to scratch my eyeballs out.” Vision should be preserved. Pain should not be severe. Photophobia should not be the main feature.
3. Watery Red Eye, Often Starting in One Eye
Think: viral conjunctivitis.
Usually there is mild discomfort, watery discharge, and sometimes upper respiratory symptoms, or even a sick contact who had a red eye. It can start in one eye and spread to the other. Vision is usually preserved. Pain is usually mild. Patients often endorse lids being stuck together when they wake up. If there is significant photophobia, reduced vision, or corneal staining, do not call it simple viral conjunctivitis.
4. Purulent Discharge
Think: bacterial conjunctivitis.
Usually vision is preserved, pupils are normal, and the cornea is not involved. Be careful with severe purulent discharge, pain, or decreased vision. Hyperacute bacterial conjunctivitis, especially gonococcal conjunctivitis, can be aggressive.
5. Gritty/Burning Discomfort, Crusting, Fluctuating Blur
Think: dry eye or blepharitis.
This is common and often annoying rather than dangerous. Look at the lid margins. Ask about lid hygiene, screen use, morning crusting, fluctuating symptoms, rosacea, and chronicity. The blur often improves with blinking or lubrication.
6. Sectoral Redness, Mild Discomfort, Normal Vision
Think: episcleritis.
This is usually less dangerous. The trap is confusing it with scleritis. Episcleritis often blanches after topical phenylephrine (so take a picture of the eye before you put phenyl in), while the deeper redness of scleritis typically does not. In clinic, this can help distinguish the two, but the bigger student-level clue is still the story: episcleritis is usually mild discomfort with normal vision, while scleritis causes deep, piercing pain, tenderness, and may threaten vision.
7. Deep, Piercing Pain, Tenderness, Possible Reduced Vision
Think: scleritis.
This is higher risk. Ask about autoimmune disease, rheumatoid arthritis, inflammatory bowel disease, vasculitis, and prior episodes. Scleritis is not just episcleritis having a dramatic day. It can threaten vision and needs escalation. It is often the first sign of an underlying rheumatologic condition too, so all first episodes warrant a work up!
8. Painful Red Eye in a Contact Lens Wearer
Think: infectious keratitis or corneal ulcer.
This is one of the biggest “do not miss” patterns. Look carefully at the cornea. Check fluorescein. Look for epithelial defect, infiltrate, opacity, or ulcer. Do not reassure yourself with “probably conjunctivitis” in a contact lens wearer with pain or photophobia.
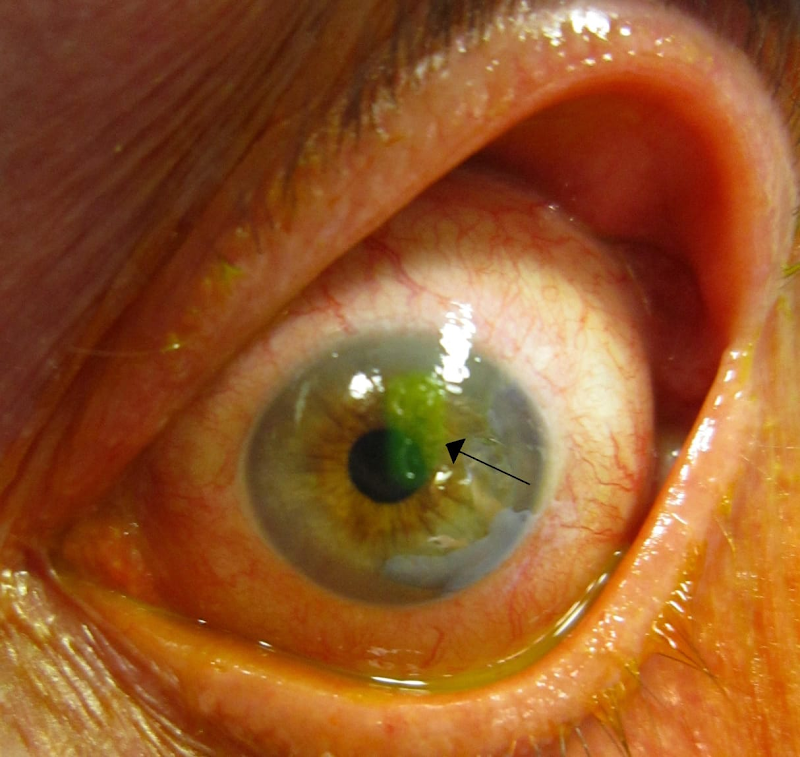
Fluorescein-stained central corneal epithelial defect in infective keratitis. Photo by MohdHaneef01, Wikimedia Commons, licensed under CC BY 4.0. Cropped for layout.
9. Branching Dendrite on Fluorescein
Think: herpetic keratitis.
Ask about prior episodes, cold sores, immunosuppression, recent illness, trauma, and sunlight exposure. Branching dendrites under fluorescein are a major clue for HSV herpetic keratitis. For active herpetic keratitis, steroids can act like pouring gasoline on a fire, management suggestions should instead focus on antivirals.
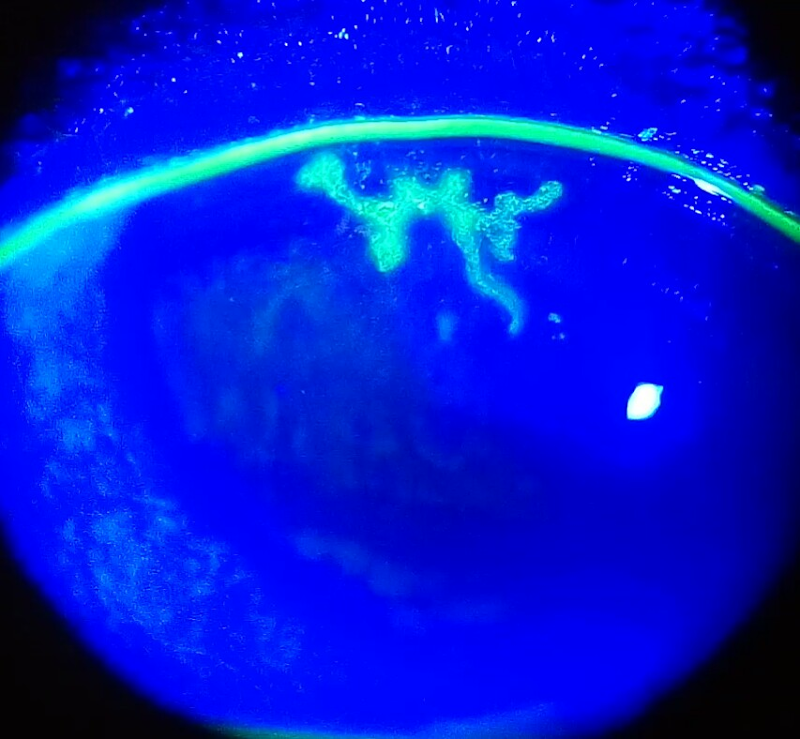
Dendritic corneal ulcer with fluorescein staining. Photo by Imrankabirhossain, Wikimedia Commons, licensed under CC BY-SA 4.0.
10. Painful Photophobic Red Eye With Ciliary Flush
Think: anterior uveitis.
Look for cell and flare. The pupil may be small or irregular if posterior synechiae are present. Ask about prior uveitis, autoimmune disease, inflammatory bowel disease, ankylosing spondylitis, sarcoidosis, infections, and systemic symptoms. This is exactly why “red eye” is too vague. The conjunctiva is red, but the problem is inside the eye.
Anterior uveitis. Photo by Gogri et al., via Wikimedia Commons, licensed under CC BY 4.0.
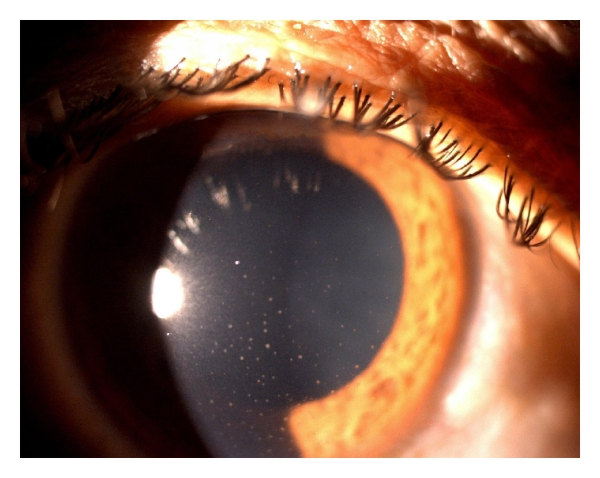
11. Severe Pain, Headache, Nausea/Vomiting, Halos, Cloudy Cornea, High IOP
Think: acute angle-closure glaucoma.
This is an emergency. The pupil may be mid-dilated and poorly reactive. The cornea may look hazy. The pressure is high. Say this one clearly when you present. Do not bury it as “maybe glaucoma?” at the end.
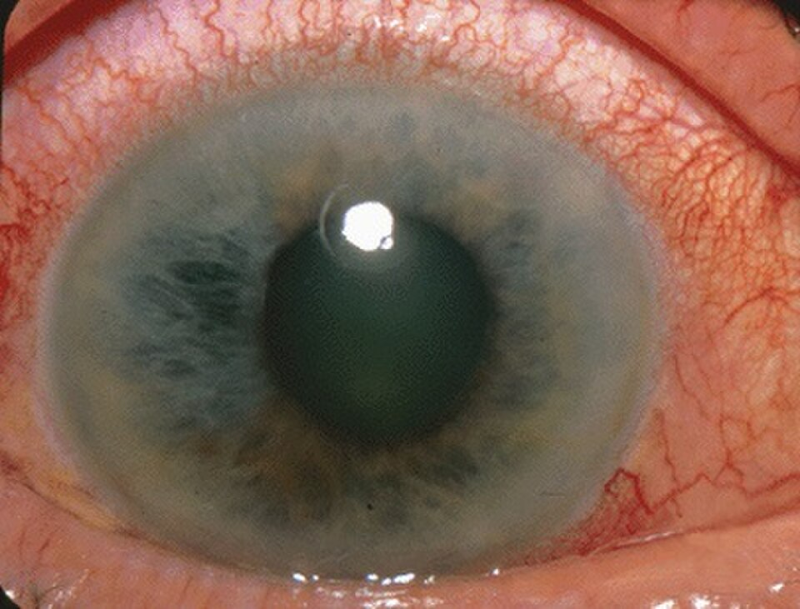
Acute angle-closure glaucoma. Photo by Jonathan Trobe, M.D., via Wikimedia Commons, licensed under CC BY 4.0.
12. Recent Surgery or Injection Plus Pain, Redness, and Decreased Vision
Think: endophthalmitis.
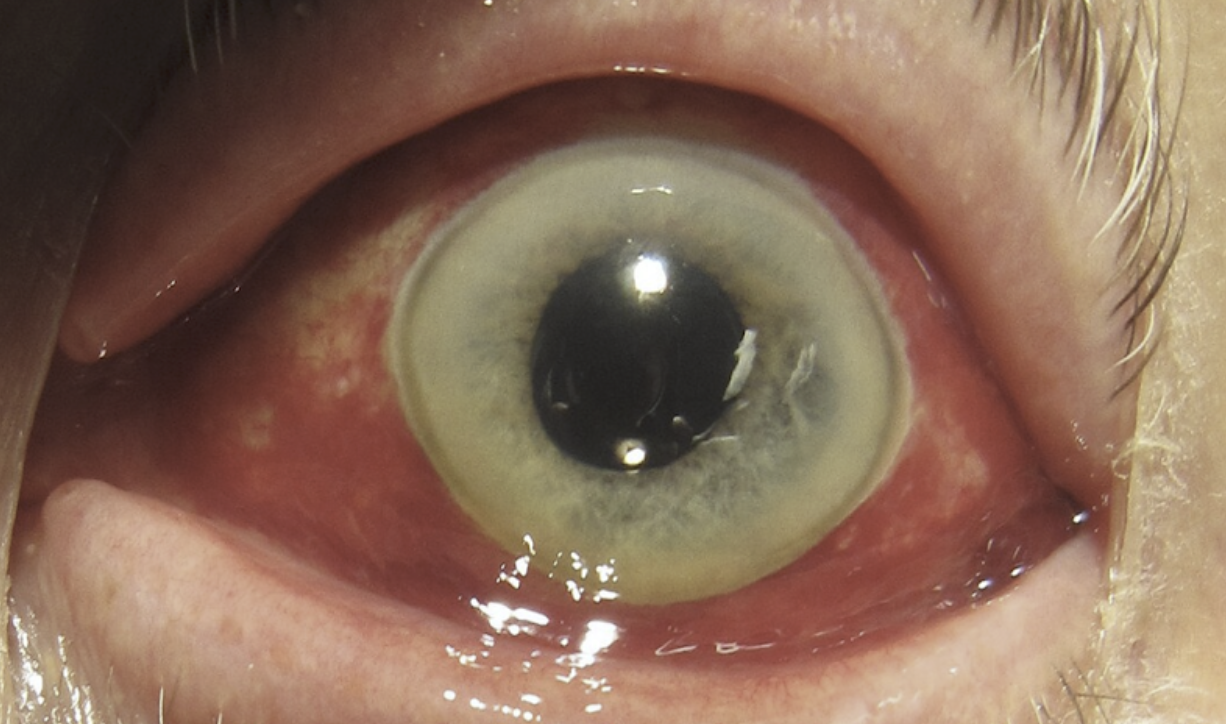
This is an emergency. Ask specifically about recent cataract surgery, intravitreal injections, trauma, or other intraocular procedures. IV drug use and bacteremia are also important risk factors! You will often see hypopyon and they need to have vitreous cells present to make the diagnosis of endophthalmitis, but you do not need to see everything to escalate the story. Recent intraocular procedure plus painful red eye plus decreased vision is enough to be very concerned. The time frame to be on high alert post injection/surgery is day 3-6. It’s possible to get endophthalmitis before and after this time frame, but most present in this window.

Endophthalmitis. Source file IMG_1380.JPG, from the eye_project dataset by Ice, via Roboflow Universe, licensed under CC BY 4.0. Cropped for layout.
Key Reminders
Remember contact lenses
Contact lens history is not optional in red eye.
A contact lens wearer with pain, photophobia, reduced vision, or corneal findings is a different risk category.
Add fluorescein
If the cornea is involved, fluorescein helps you see the problem.
Abrasions, ulcers, dendrites, and epithelial defects matter.
Check the lids
Foreign bodies hide. Follicular and papillary conjunctivitis look different and point to different sources. Flip the lid.
Check for recent surgery or injection
Post-op or post-injection red eye is not routine until someone appropriate has decided it is routine.
If You Remember Nothing Else
Red eye is common. Dangerous red eye is less common, but you cannot afford to miss it.
Ask:
Check:
Then ask yourself:
Could this threaten vision?
If yes, say that clearly.
You do not need to diagnose every red eye perfectly. You need to recognize when the eye is angry enough to deserve urgent help.
Next month:
Flashes, Floaters, and Visual Disturbances


