
Authored by Nicholas Oliver Corey Kuzik
Reviewed by Stephen Carrell, PGY-4 at University of Alberta
Edited and posted by Yosra Er-reguyeg
May 23, 2026 | 5 min

I hear a patient is coming in complaining of vision loss.
What could be worse than that??
It's enough to make me jump out of my seat, ready to spring into action...but maybe springing a bit too quickly because I get a bout of orthostatic hypotension. Or transient, painless, binocular vision loss from standing up too fast. Am I the patient now? Nope, still the med student, just a little more dizzy than usual.
Lesson learned: Vision loss has a massive differential & you spring into action at a reasonable speed.
A patient may say they “lost vision” when they mean blur, darkness, distortion, double vision, a missing patch, a curtain, trouble reading, washed-out colours, or a few seconds of greying out when they stand up too quickly.
So, before panicking, the first step is to translate the complaint into a system that can help narrow the diagnosis.
Start by Making “Vision Loss” Less Vague
When someone says their vision is worse, slow down and clarify what they mean.
Ask:
Now that we have characterized the vision loss, we can ask about possible precipitating events that continue to narrow the differential:
Blurry eyes after a long day of meticulously editing your vision loss decision tree is very different from sudden painless monocular vision loss in a patient with vascular risk factors.
Still vision loss or change. Very different level of panic.
Use the Decision Tree, But Don’t Worship It
The figure below is meant to help organize the differential for true vision loss, dimming, or field loss.
It is not meant to cover every visual symptom. Distortion, diplopia, flashes, floaters, halos, and photopsias deserve their own approaches and will be covered in future posts.
The key questions are:
That is already enough to get you moving in the right direction.
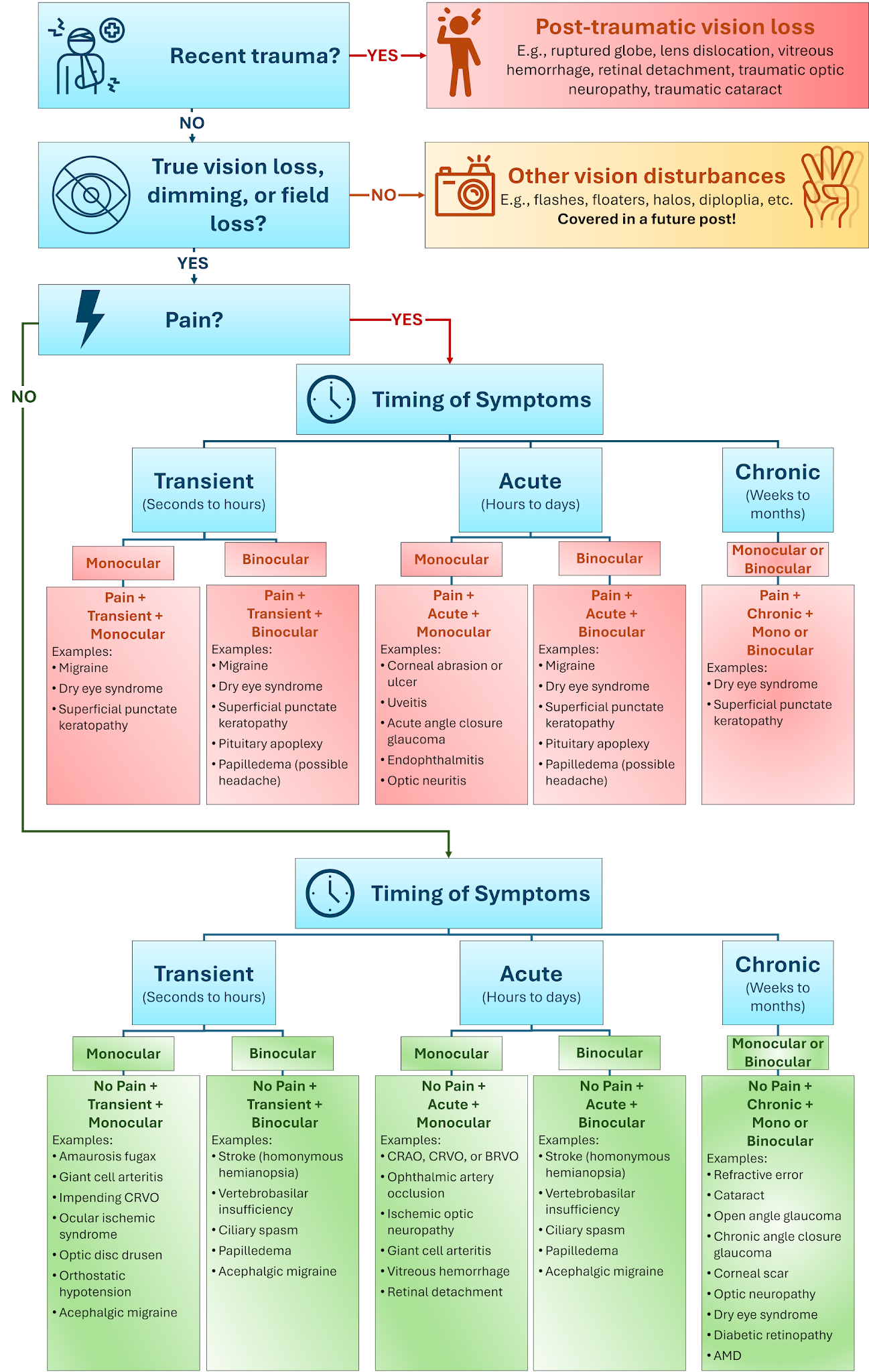
The point of the figure is not to memorize every diagnosis. It is to help you ask better questions before you start guessing. This is a great starting point for organizing your differentials. As you gain experience in diagnosing all the various causes of vision loss your “decision tree” will change.
First: Was There Recent Trauma?
If there was trauma to the eye or head, take that seriously and shift into a trauma pathway.
Post-traumatic visual loss can come from almost anywhere along the visual system:
The big mistake students make is treating trauma as a minor detail. It is not. If there is trauma plus decreased vision (and other red flag signs of a globe rupture), your job is to communicate that clearly. Also, remember the major safety rule from Part 1: if you are worried about an open globe, do not check pressure. That is a good way to turn a bad day into a worse one.
Is This True Vision Loss?
Patients, and sometimes referring doctors, often use “vision loss” as shorthand for any visual disturbance.
Before you build a huge differential, figure out whether they mean true loss of vision, dimming, or field loss — or whether they mean something else.
Examples of “something else” include:
These symptoms are still important. They are just different pathways. For this post, we are focused on true vision loss, dimming, or field loss. If the patient is describing distortion, think macula. If they are describing double vision, think of refractive issues, alignment, or neurologic pathways. If they are describing flashes, floaters, or a curtain, think vitreous and retina.
This is why “blurry vision” is never enough. You need to make the complaint specific.
Pain or No Pain?
Once you know you are dealing with true vision loss, pain is one of your most important forks.
Painful vision loss
Painful vision loss is never benign until proven otherwise. That does not mean every patient with pain and blurry vision has a catastrophe happening. But it does mean you should slow down and collect better data, before calling it a migraine or dry eye.
Painful vision loss can point toward:
Pain tells you the eye is angry. Vision loss tells you the anger may be affecting important structures. That combination deserves respect.
Painless vision loss
Painless vision loss can be dangerous in a quieter way. Patients may look calm. The eye may look white. You may not get the emotional cue that something serious is happening.
Painless vision loss can point toward:
Painless does not mean safe. Sometimes, painless vision loss is the most time-sensitive presentation in the room.
Timing: Transient, Acute, or Chronic
The next major question is timing.
Transient vision loss
Transient vision loss is easy to dismiss because the patient may look completely normal by the time you see them. Do not dismiss it.
Ask:
Transient monocular vision loss can be amaurosis fugax until proven otherwise. In the right patient, it may be a warning sign for vascular disease and provides an opportunity to reduce the risk of serious ischemic events to the eye(s) or brain by starting or increasing anti-platelet therapies. Brief episodes of dimming, greying out, or blacking out of vision are often called transient visual obscurations (TVOs). When they are triggered by posture change, bending, or Valsalva, especially with headache or pulsatile tinnitus, think about increased intracranial pressure. Migraine aura is common, but it should be something you arrive at after asking the right questions, not a reflexive shrug.
Acute vision loss
For this decision tree, think of acute as roughly within hours to a couple of days.
Acute vision loss should make you pause, especially when it is sudden, painless, and monocular.
That pattern should make you think about:
The exact diagnosis matters, but the first move is recognizing the urgency. A patient with sudden painless monocular vision loss is not someone you casually add to the bottom of a list.
Chronic vision loss
Chronic vision loss is often less emergent, but still important. A good question to ask is why they came in today? Why not earlier?
Think about:
Gradual does not usually mean “minutes matter.” But it also does not mean “ignore it.” The key is identifying whether there are red flags hiding inside the gradual story.
For example:
Monocular or Binocular?
Patients are not always reliable when they say “both eyes.” They may mean:
So check by covering each eye individually if presenting with current visual changes, or ask them about their symptoms when the past vision loss was occurring:
“If you covered one eye, was the problem still there? What about if you had covered the other eye?”
Monocular vision loss
Monocular vision loss usually points you toward the eye or optic nerve (anterior to the chiasm):
Examples include corneal ulcer, keratoconus, cataract, vitreous hemorrhage, retinal detachment, CRAO, and optic neuritis.
Binocular vision loss
Binocular symptoms suggest pathology posterior to the chiasm (but don't forget simultaneous pathology bilaterally anterior to the chiasm!):
This is also where patients may actually be describing diplopia, not vision loss. If covering either eye makes the problem go away, that is binocular diplopia, not true binocular vision loss. Diplopia is a different pathway in our differential, and will be covered in a future blog.
The Patterns You Should Start Recognizing
You do not need to memorize every diagnosis in the figure. Start by recognizing the patterns.
Acute + painless + monocular
This is one of the highest-stakes branches:
Examples include CRAO, CRVO, ischemic optic neuropathy, GCA, vitreous hemorrhage, and retinal detachment.
A strong student presentation might sound like:
“This is a 68-year-old with known HTN and T2DM, complaining of acute painless monocular vision loss in the right eye starting one hour ago in the absence of trauma. Vision is counting fingers. There is a RAPD. I’m concerned about a retinal vascular event, especially CRAO. I think we should do an urgent dilated fundus examination, with OCT or fundus imaging if available.”
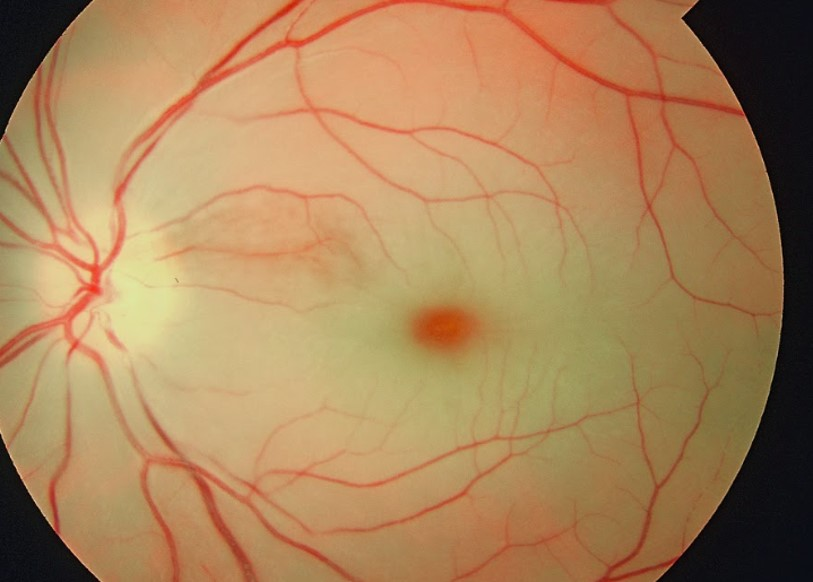
Image: Dr. Gopal Bisht, Cherry red spot in patient with central retinal artery occlusion (CRAO), Wikimedia Commons, 2019, licensed under CC BY-SA 4.0.
Transient + painless + monocular
This is the “do not be falsely reassured because it resolved” branch:
The scary version is an older patient with transient monocular vision loss and headache, jaw claudication, scalp tenderness, etc. This should point you towards GCA (though, even without the classic GCA symptoms, this should be high on your differential). The patient’s vision may be normal when you see them. That does not mean the story is harmless.
Acute + painful + monocular
This branch often points you to the front of the eye, high pressure, infection, or the optic nerve:
Context matters! A painful red eye in a contact lens wearer is different from a painful eye with decreased colour vision and pain on eye movements. A post-operative eye with pain and decreased vision is different again. Do not let “painful eye” be the final description. Keep going.
Acute or transient + binocular
This branch should make you think more neurologically:
Your history needs to expand beyond the eye. Make sure to ask about weakness, numbness, speech difficulty, headache, nausea/vomiting, TVOs, and diplopia. Sometimes the eye complaint is the canary in the coal mine for neurologic diagnosis.
Chronic + painless
This is often the lower-drama branch, but still a high-volume one:
These may not be emergency consults, but they are still important. Your job is to identify whether the story is truly chronic and stable, or whether the patient has an acute change layered on top of a chronic baseline.
The Exam You Need
For vision loss, do not overcomplicate your first pass. Start with the basics from Part 1.
Vision
Pupils
Pressure
Anterior segment
Fundus
Try to comment on:
And if you cannot see the fundus, say that. A poor view is a finding.
How to Present Vision Loss
A strong vision loss presentation should include:
Example:
“This is a 72-year-old with acute painless monocular vision loss in the left eye starting this morning. Vision is hand motion OS and 20/25 OD. There is an RAPD on the left. IOP is normal. The cornea is clear and the eye is quiet. I’m concerned about CRAO or ischemic optic neuropathy, and given the age I would also want to ask carefully about GCA symptoms.”
That is useful.
Another example:
“This is a 34-year-old female with two days of painful vision loss in the right eye, worse with eye movements. Vision is 20/80 OD and 20/20 OS. Colours are washed out on the right and there is an RAPD. An ishihara test revealed reduced color vision OD with 1/17OD and 17/17OS. I’m concerned about optic neuritis.”
Again, you might not be right.
But you are showing your reasoning.
That is the point.
If You Remember Nothing Else
For vision loss, ask:
Then check:
And always ask yourself:
“Could this threaten vision or life if I miss a key diagnostic clue?”
Next month:
Red Eye on Your Ophthalmology Elective


